Initial situation and objectives
For 75 years, the Constitution of the World Health Organization (WHO) has defined ‘health’ not merely as the absence of disease, but as a ‘state of complete physical, mental and social well-being’ (WHO, 1946). The WHO’s definition certainly isn’t undisputed. However, it does present an opportunity to gain a better understanding of both increasing health inequality and the social aspects of health in general.
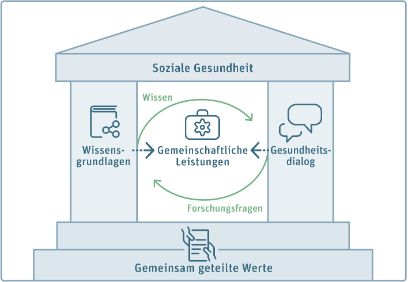
Experts from three universities and from the Federal Office of Public Health (FOPH) have compiled different perspectives on the social aspects of health and transformed them into a common, interdisciplinary definition.
The shared objective of establishing a definition for ‘social health’ was based on the belief that, in order to develop public health, greater focus must be placed on social aspects. The results of this process, which lasted several days, will be published on this website and presented for discussion.
‘My research focuses on the role of religious models of interpretation in vaccine-sceptical discourse. This issue is inextricable from the context of the public and media arenas in which social health is negotiated. This workshop allowed me to engage constructively with a very topical issue in a highly interdisciplinary context.’
Ass. Prof. Andrea Rota
‘When it comes to health promotion, it’s important to establish a common understanding of social health in terms of social quality of life and cohesion. The workshop provided an opportunity to define this term in an interdisciplinary and transdisciplinary context.’
Dr. Sebastian Mader
References, bibliography
- Knapp, J., Zeratsky, J., & Kowitz, B. (2016). Sprint: How to Solve Big Problems and Test New Ideas in Just Five Days (1st edition). Redline Verlag.
- Max-Neef, M. A. (ed.). (1991). Human scale development: Conception, application and further reflections. Apex press.
- Obrecht, W. (2005). Umrisse einer biopsychosoziokulturellen Theorie menschlicher Bedürfnisse: Geschichte, Probleme, Struktur, Funktion. [Outline of a biopsychosociocultural theory of human needs: History, Problems, Structure, Function]. Zurich. Hochschule für Soziale Arbeit.
- Pauls, H. (2004). Klinische Sozialarbeit: Grundlagen und Methoden psycho-sozialer Behandlung. (Grundlagentexte soziale Berufe) [Clinical Social Work: Foundations and Methods of Psycho-Social Treatment. (Fundamental texts on social professions)]. Juventa-Verlag.
- Pfaff, H., Ernstmann, N., Driller, E., Jung, J., Karbach, U., Kowalski, C., Nitzsche, A., & Ommen, O. (2011). Elemente einer Theorie der sozialen Gesundheit [Elements of a social health theory]. In Gesundheit und Gesellschaft [In Health and Society]. Die Gesellschaft und ihre Gesundheit: 20 Jahre Public Health in Deutschland / Bilanz und Ausblick einer Wissenschaft [Society and its health. 20 years of public health in Germany/Review and outlook of a science] (pp. 39– 68). VS Verlag für Sozialwissenschaften.
- WHO. (1946). Constitution of the World Health Organization. New York. WHO.